





Gestational diabetes mellitus (GDM) has been extensively studied due to its wide-reaching impact on maternal and foetal health. However, emerging research has begun to focus on its less visible consequences, particularly the subclinical changes it induces in maternal heart function. A recent systematic review and meta-analysis published in the European Journal of Obstetrics & Gynaecology examines the link between GDM and subclinical myocardial dysfunction, focusing on global longitudinal strain (GLS) as a marker of heart health.
The study analyzed data from 10 different studies involving a total of 1147 women with GDM and 7706 healthy pregnant controls. Using speckle tracking echocardiography (STE), the researchers found that women with GDM showed significant reductions in left ventricular global longitudinal strain (LV-GLS) compared to healthy pregnant women. The overall standardized mean difference (SMD) in GLS between GDM patients and controls was -0.97, indicating a substantial subclinical impairment in myocardial function among the GDM population.
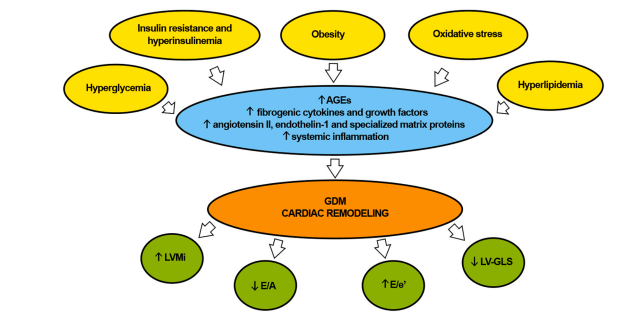
Fig. 1. Pathophysiologic mechanisms of cardiac remodeling in GDM women. Even a short period of exposure to hyperglycemia during pregnancy, insulin resistance
and hyperinsulinemia, obesity, oxidative stress and hyperlipidemia may lead to the formation of AGEs and may activate cardiac fibroblasts and other myocardial cell
types, such as cardiomyocytes, immune cells and vascular cells. These cells, in turn, may release several fibrogenic cytokines and growth factors, may induce v
activation of angiotensin II, endothelin-1 and specialized matrix proteins and may increase systemic inflammation, thus promoting myocardial stiffness in diabetic
mothers. GDM cardiac remodeling is characterized by cardiomyocyte hypertrophy, leading to an increase in LV mass, to an early decline in diastolic function and
concurrent changes in myocardial deformation indices, which commonly precede systolic dysfunction. AGEs, advanced glycation end products. GDM, gestational
diabetes mellitus.
The importance of this finding cannot be overstated, as LV-GLS is a sensitive marker of early heart dysfunction that precedes overt changes in heart geometry and pump function. In women with GDM, even though traditional echocardiographic measures like ejection fraction (LVEF) remained within normal ranges, the reduced LV-GLS points to subtle myocardial impairment. This could have long-term implications, potentially increasing the risk of developing cardiovascular diseases later in life.
Despite significant heterogeneity across the studies in terms of sample sizes, diagnostic criteria, and demographics, the review consistently demonstrated that GDM independently contributed to subclinical myocardial dysfunction. No significant publication bias was detected, which adds robustness to the study’s conclusions.
Given these findings, the authors advocate for the use of speckle tracking echocardiography as a diagnostic tool to monitor heart function in women with GDM. Early identification of those at risk for myocardial dysfunction could allow for timely interventions—both pharmacological and lifestyle-related—that may mitigate the long-term cardiovascular risks associated with GDM. The findings also emphasize the need for broader public health strategies to manage GDM and its potential consequences beyond pregnancy, particularly in reducing the future risk of type 2 diabetes and cardiovascular disease.
In conclusion, while GDM is traditionally associated with perinatal outcomes, this study provides critical insights into its role in subclinical cardiac dysfunction. As our understanding of the metabolic and cardiovascular links between pregnancy and later health evolves, this research underscores the importance of vigilant cardiovascular monitoring and early intervention for women affected by GDM.
Journal Article: Sonaglioni, A., Bordoni, T., Naselli,(et. al), (2024). The influence of gestational diabetes mellitus on subclinical myocardial dysfunction during pregnancy: A systematic review and meta-analysis. European Journal of Obstetrics, Gynecology, and Reproductive Biology, 292, 17–24.
Summary by Faith Oluwamakinde



