





- Patient Presentation
- History
- Differential Diagnosis
- Examination
- Investigations
- Discussion
- Treatment
- Final Outcome
- References
- Evaluation - Questions & Answers
- MCQ
Patient Presentation
A 53 year old male, originally from India, presented to the clinic for a renewal of his hypertension medication. On routine weighing it was noted that he had lost 8 kg in the last 6 months, which had been unintentional weight loss. Other then some mild lower abdominal pain, and some occasional testicular discomfort, he reported no other symptoms.
Acknowledgement
This case study was kindly provided by Dr Monica Mercer, MBChB from Immunopaedia
History
The patient had been diagnosed with hypertension 6 years before and had remained well controlled during this time attending clinic regularly for his 6 monthly check up and medication.
Although he had occasional mild abdominal pain over the last 6 months there was no accompanying vomiting or constipation but he did report some bouts of nausea. However no trigger was noted, and no particular frequency was observed. The 8kg weight loss had been unintentional, with no loss of appetite noted.
No urinary symptoms were reported including no dysuria, no retention, no frequency, no urgency, no nocturia and no haematuria.
On further questioning his testicular discomfort had been noted in both testes, with more tenderness on the right side. The testicles had increased in size slowly, but because they were not particularly painful the patient was not concerned. There was no penile involvement and sexual function was not affected. Infertility was of no consequence, he has 3 children aged 24, 27 and 30 years and he and his wife of 32 years had conceived easily and had not tried for further pregnancies.
Past medical history
An incomplete history was given of a diagnosis of Pulmonary TB 12 years earlier while still living in India. Although he was treated for TB he does not know what medication he was given, and treatment was only for four months. He remembers submitting a sputum specimen at four months, after which his treatment was ended. Thereafter no further follow up was done.
His hypertension was diagnosed on a routine medical check up 6 years ago when he moved to South Africa. He has been on treatment since diagnosis and has remained well controlled.
A routine investigation for HIV was carried out 6 months ago for insurance purposes and was found to be negative.
Past Surgical History
No previous surgery
Family History
Father and mother are both hypertensive and on treatment. No other significant family history.
Social History
20 year pack history of smoking
No alcohol intake
Differential Diagnosis
- Epididymitis
- Hydrocoele
- Spermatocoele
- Neoplasm
- Tuberculoma
Examination
Vitals
- Blood pressure 138/85
- Heart rate 88
- Respiratory rate 18
- Temperature 36°C
- Oxygen saturation 99% on room air
General
- No signs of dehydration
- No jaundice
- No pallor
- No oedema
- No stigmata of HIV
Respiratory
- No signs of respiratory distress
- Chest clear, good air entry bilaterally
Cardiovascular
- All pulses present, normal rate, rhythm and character
- No raised JVP
- Apex beat normally placed
- No palpable P2, no parasternal heave, no thrills
- S1, S2 present, no murmurs
Abdomen
- Non distended
- Soft and non tender
- No organomegaly
- Bowel sounds present
Genitourinary
- Penis appears normal, no overlying skin lesions, no discharge.
- Scrotum noted to have normal overlying skin, no lesions, sinuses or erythema.
- Testes are notably enlarged, right side 10×10 cm and left side 8x7cm.
- On palpation the right testis is enlarged with some swelling noted on the extratesticular inferior surface and in the spermatic cord. The enlargement is somewhat irregular, firm with mild tenderness. The left testis was similarly enlarged but no spermatic cord involvement was felt.
- No hernias or hydrocoele were found.
Neurological
- Higher function intact, orientated to person, place and time
- No signs of neck stiffness or meningism
Gait
- Normal
Cranial nerves
-
- All cranial nerves normal function
Power
-
-
- Globally 5/5
-
Tone
-
-
- Globally normal tone
-
Reflexes
-
-
- Globally – 2/4
-
Sensation
-
-
- Globally intact
-
Investigations
Chest X ray, shows small cavity in the right upper lobe, and small area of calcification in the right middle lobe most likely a Ghon focus- in keeping with his previous history of pulmonary TB
| Examination | Value | Normal Limits |
|---|---|---|
| WBC | 4.8 | (4-12 x109/L) |
| HB | 12.8 | (12.1-15.2 g/L) |
| Platelets | 240 | (140-450 x109/L) |
| CRP | 5 | (0-8mg/l) |
| NA | 138 | (135-147 mmol/L) |
| K | 4.5999999999999996 | (3.3-5.0 mmol/L) |
| CL | 100 | (99-103 µmol/L) |
| C02 | 26 | (18-29 mmol/L) |
| Urea | 5.2 | (2.5-6.4 mmol/L) |
| Creatinine | 101 | (62-115 mmol/L) |
| Total protein | 65 | (60-80g/L) |
| Albumin | 38 | (35-50g/L) |
| Corrected Calcium | 2.4700000000000002 | (2.1-2.6mmol/l) |
| Phosphate | 1.35 | (1.0-1.5 mmol/l) |
| Magnesium | 0.89 | (0.8-1.3) |
| Tumor Markers | ||
| a - feto protein | 1 | (1.0-4.0) |
| bHCG | negative | |
| HIV Elisa | non reactive |
-
-
- A urine culture was negative for bacteria and AFB negative.
-
- Ultrasound of scrotum demonstrated enlarged testes, with right testicle larger then left. Both testicles were shown to have a well-defined hypoechoic mass with foci of calcifications. Magnetic resonance imaging (MRI) confirmed these findings.
-
- Histological investigations of ultrasound guided core biopsies from both testicles detected the presence of caseating granuloma and Ziehl–Neelsen staining of slides from both biopsies demonstrated acid-fast bacilli.
-
Discussion
Extra Pulmonary TB
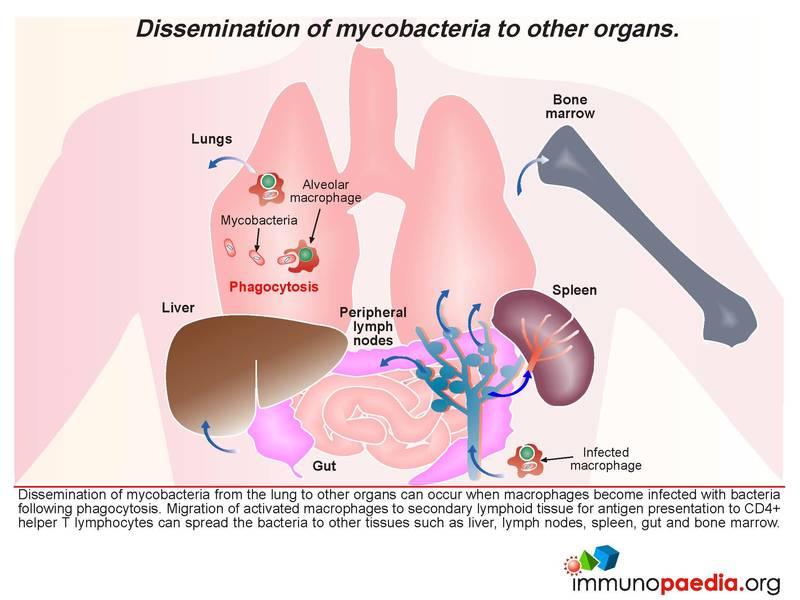
This case study explores the immunological manifestation of extra pulmonary TB. Although the lung in pulmonary TB is the most common site for Mycobacterium tuberculosis infections, dissemination of mycobacteria from a primary lung infection to other organs can occur when alveolar macrophages become infected with bacteria following phagocytosis. Mycobacteria have evolved adaptive mechanisms to evade destruction in macrophages and can survive in vacuoles. Migration of activated macrophages to secondary lymphoid tissue for antigen presentation to CD4+ helper T cells can facilitate spread of mycobacteria to other tissues such as the pleura, liver, lymph nodes, spleen, gut, bone marrow, brain and the urogenital tract. In immunocompetent hosts, mycobacterial dissemination to other tissues is usually controlled. However, due to the testis being an immune privileged site, it is likely that intracellular mycobacteria may have a survival advantage in this tissue.
In this case study, our patient was previously infected with pulmonary TB, which was treated but possibly sub-optimally. His history was incomplete and opened questions to whether previous treatment was curative. It is possible that our patient was latently infected with TB and we assume that reactivated mycobacteria disseminated to the testes.
Pathophysiology
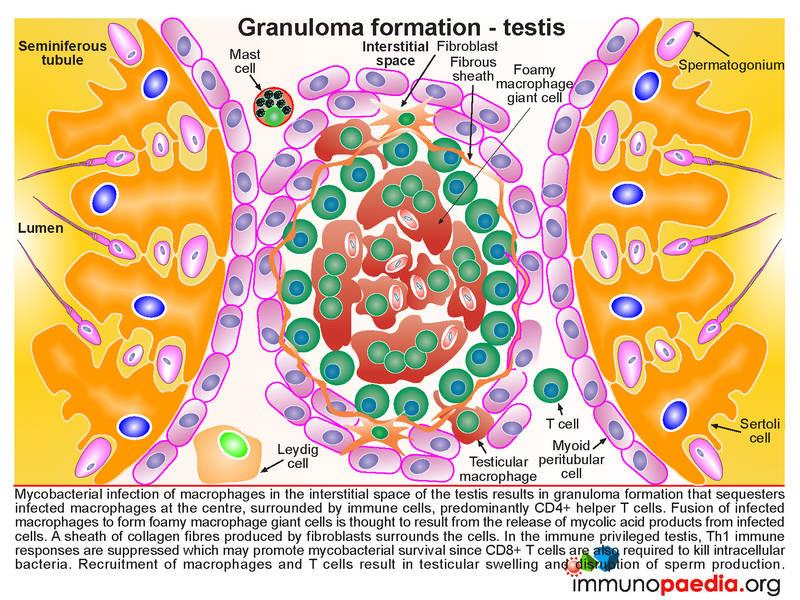
We outline below the main points about the pathology of extra-pulmonary testicular TB. Following infection of the testicular macrophages located in the interstitial space of the testis with mycobacteria, the infected cells promote an immune response which results in the formation of a granuloma . This serves to sequester infected cells at the centre surrounded by predominantly CD4+ helper T cells. The infected macrophages can fuse to form foamy macrophage giant cells, which are thought to result from mycolic acid products released from infected cells. A sheath of collagen fibres produced by fibroblasts then surrounds the cells.
In the immune-privileged testis, Th1 immune responses are suppressed and it is thought that this suppression promotes mycobacterial survival because CD8+ T cells which are required to kill intracellular bacteria are not recruited. Th1 helper T cells provide essential cytokine activation signals to CD8+ cytotoxic T cells. The build up of recruited macrophages and T cells is thought to result in progressive testicular swelling and disruption of sperm production. As noted in our patient there was development of gradual testicular enlargement. Whether this resulted in infertility is not known, as the patient originally became infected with TB after having children.
Immune Privileged Sites
Apart from the testis, other immune privileged sites include the eye, brain and placenta and are so-called because of mechanisms of immune tolerance that operate to protect the tissues from immune-mediated damage. The following discussion we will focus on the testis.
Blood-testis Barrier
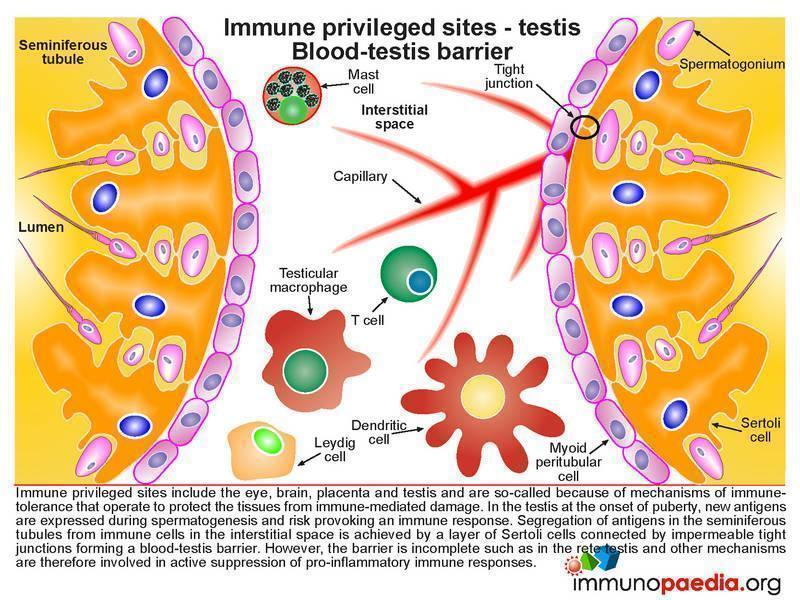
In thetestis at the onset of puberty, new antigens are expressed during spermatogenesis and risk provoking an immune response because their development occurs after immune tolerance has been established. Mechanisms must therefore be in place to protect them. This is achieved in part by segregation of antigens in the seminiferous tubules from immune cells in the interstitial space by a layer of Sertoli cells connected by impermeable tight junctions which form a blood-testis barrier. However this physical barrier cannot account for all immune suppression in the testis because it is incomplete in the region called the rete testis, thus allowing for some exposure to antigen.. Thus other forms of immune suppression mechanisms are in place.
Immune Evasion
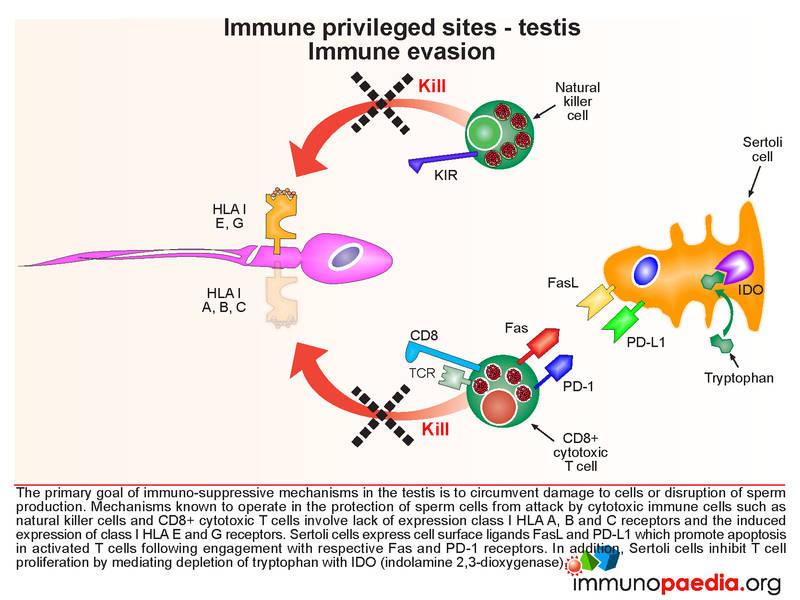
The primary goal of immune suppressive mechanisms in the male testis is to circumvent destruction of testicular cells or disruption of sperm production. Mechanisms known to operate in the protection of sperm cells from attack by cytotoxic immune cells such as natural killer cells and CD8+ cytotoxic T cells involve lack of expression of classical HLA class I A, B and C receptors and the induced expression of non-classical HLA E and G receptors. Sertoli cells also express cell surface ligands FasL and PD-L1 which promote apoptosis in activated T cells following engagement with their respective Fas and PD-1 receptors. In addition, Sertoli cells which are support cells, inhibit T cell proliferation by mediating depletion of tryptophan with IDO (indolamine 2,3-dioxygenase). Lack of tryptophan inhibits protein synthesis in activated T cells.
Immune Deviation
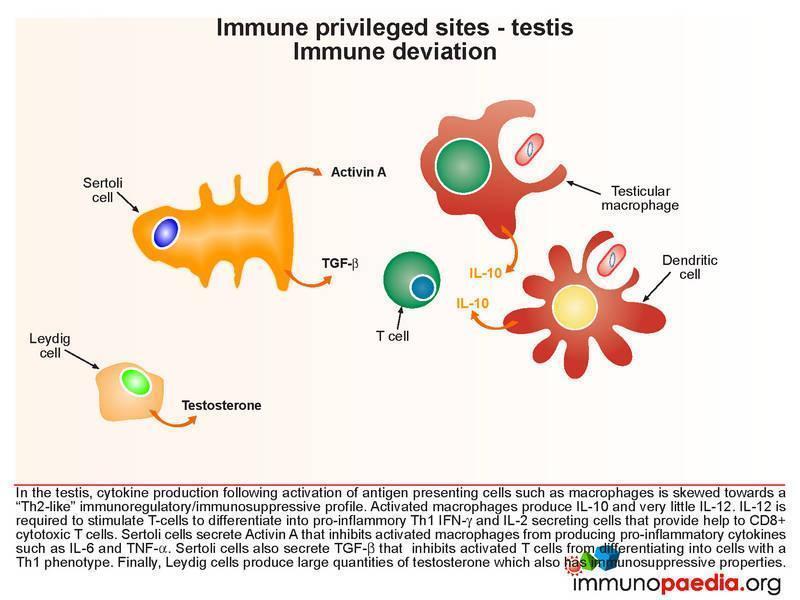
In the testis, cytokine production following activation of antigen presenting cells such as macrophages is skewed towards a “Th2-like” immunoregulatory /immunosuppressive profile. Activated macrophages produce IL-10 and very little IL-12. IL-12 is the cytokine required to stimulate T-cells to differentiate into pro-inflammatory Th1 IFN-g and IL-2 secreting cells. Th1 helper T cells necessary to provide activation signals to CD8+ cytotoxic T cells. IL-10 is also a potent inhibitor of Th1 helper T cells and antagonize the production of IFN-g production. Additionally, Sertoli cells secrete Activin A that inhibits activated macrophages from producing pro-inflammatory cytokines such as IL-6 and TNF-a. Sertoli cells also secrete TGF-b that inhibits activated T cells from differentiating into cells with a Th1 phenotype. Finally, Leydig cells produce large quantities of testosterone which also has immunosuppressive properties. Due to the local production of testosterone in the testis, testosterone levels can be up to 10 fold greater than observed on blood.
Download images for this case
Treatment
Lets go back to our patient. He was put on treatment for extrapulmonary TB with Rifampicin, Isoniazid, Ethambutol and Pyrozinamide, followed by seven months of maintenance therapy with Rifampicin and Isoniazid.
Download images for this case
Final Outcome
The patient is currently on maintenance therapy. The testicles decreased in size as a result of the testicular macrophages decreasing their burden of bacteria and a reduction in chemotactic recruitment of immune cells into the testicle.
Download images for this case
References
Meinhardt, A et al. (2010). Immunological, paracrine and endocrine aspects of testicular immune privilege. Mol Cell Endocrinol. Apr 2.
Cheng X et al. (2009). Interaction of programmed death-1 and programmed death-1ligand-1 contributes to testicular immune privilege. Transplantation. Jun 27;87(12):17
Download images for this case
Evaluation – Questions & Answers
What is the diagnosis?
What is an immune privileged site?
What immune response is suppressed in the immune privileged testis and how does this effect mycobacterium infection?
Why are sperm cells immunogenic?
What is the blood-testis barrier?
What are some of the other immune suppression mechanisms in place to help contribute to the testis being an immune privilege site?
- Lack of expression of classical HLA class I A, B and C receptors
- Induced expression of non-classical HLA class I E and G receptors
- Expression of cell surface ligands FasL and PD-L1 on Sertoli cells which promote apoptosis in activated T cells
- TGF-b secretion by Sertoli cells inhibit Th1 T cell activation
- IDO expression by Sertoli cells depletes tryptophan and inhibits T cell proliferation
- Activin A secretion by Sertoli cells inhibits activated macrophages from secreting pro-inflammatory cytokines
- Activated macrophages produce IL-10 and very little IL-12 thus preventing T-cells from differentiating into pro-inflammatory Th1 IFN-g secreting cells
Download images for this case
Multiple Choice Questions
Earn 1 HPCSA or 0.25 SACNASP CPD Points – Online Quiz
Download images for this case



